Across the United States, and the world, the coronavirus seems to be loosening its stranglehold. The deadly curve of cases, hospitalizations and deaths has yo-yoed before, but never has it plunged so steeply and so fast.
Is this it, then? Is this the beginning of the end? After a year of being pummeled by grim statistics and scolded for wanting human contact, many Americans feel a long-promised deliverance is at hand.
We will win against the virus and regain many aspects of our pre-pandemic lives, most scientists now believe. Of the 21 interviewed for this article, all were optimistic that the worst of the pandemic is past. This summer, they said, life may begin to seem normal again.
But — of course, there’s always a but — researchers are also worried that Americans, so close to the finish line, may once again underestimate the virus.
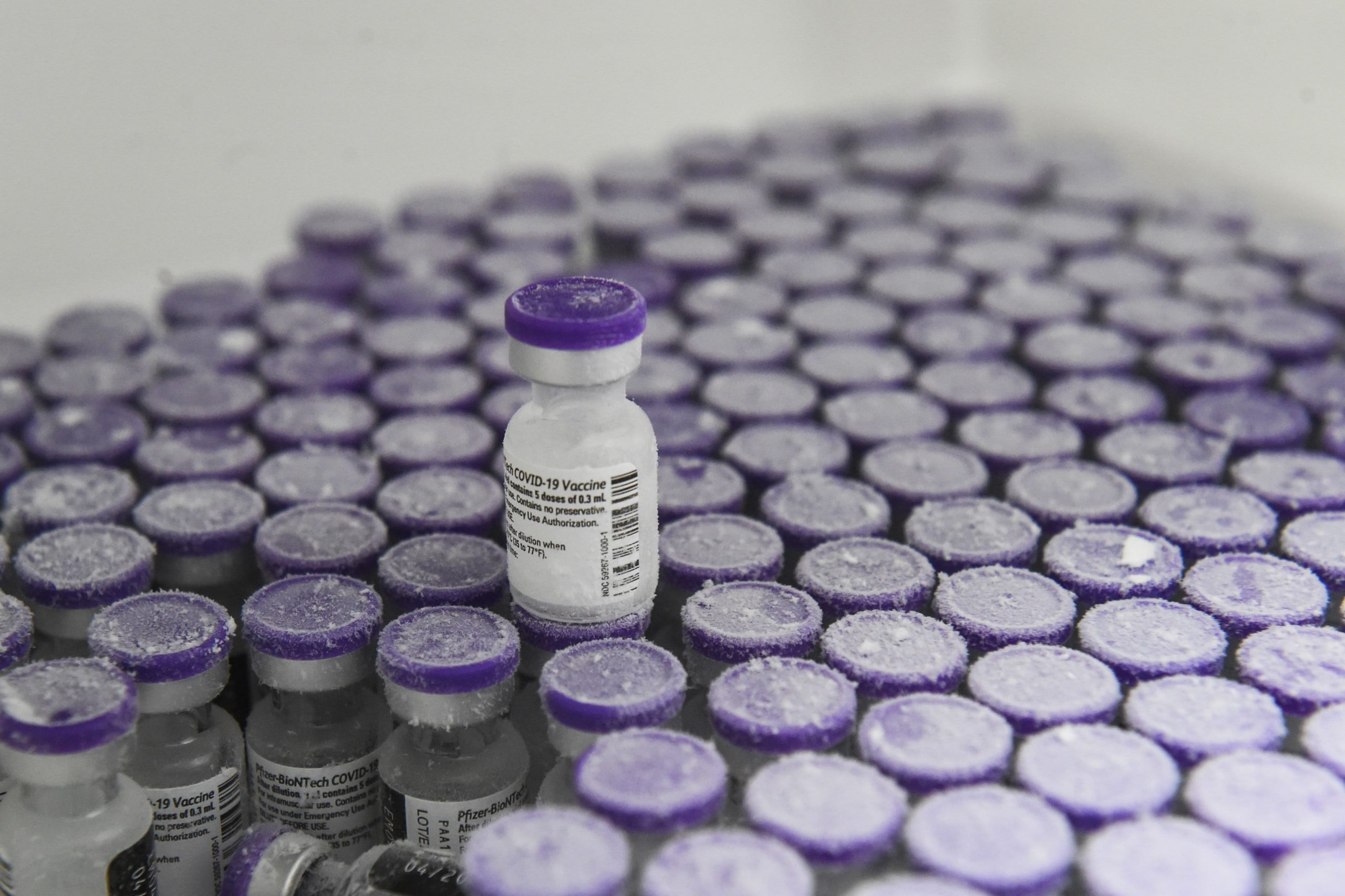
So far, the two vaccines authorized in the United States are spectacularly effective, and after a slow start, the vaccination rollout is picking up momentum. A third vaccine is likely to be authorized shortly, adding to the nation’s supply.
But it will be many weeks before vaccinations make a dent in the pandemic. And now the virus is shape-shifting faster than expected, evolving into variants that may partly sidestep the immune system.
The latest variant was discovered in New York City only this week, and another worrisome version is spreading at a rapid pace through California. Scientists say a contagious variant first discovered in Britain will become the dominant form of the virus in the United States by the end of March.
The road back to normalcy is potholed with unknowns: how well vaccines prevent further spread of the virus; whether emerging variants remain susceptible enough to the vaccines; and how quickly the world is immunized, so as to halt further evolution of the virus.
But the greatest ambiguity is human behavior. Can Americans desperate for normalcy keep wearing masks and distancing themselves from family and friends? How much longer can communities keep businesses, offices and schools closed?
Covid-19 deaths will most likely never rise quite as precipitously as in the past, and the worst may be behind us. But if Americans let down their guard too soon — many states are already lifting restrictions — and if the variants spread in the United States as they have elsewhere, another spike in cases may well arrive in the coming weeks.
Scientists call it the fourth wave. The new variants mean “we’re essentially facing a pandemic within a pandemic,” said Adam Kucharski, an epidemiologist at the London School of Hygiene and Tropical Medicine.
The declines are real, but they disguise worrying trends.
The United States has now recorded 500,000 deaths amid the pandemic, a terrible milestone. As of Wednesday morning, at least 28.3 million people have been infected.
But the rate of new infections has tumbled by 35 percent over the past two weeks, according to a database maintained by The New York Times. Hospitalizations are down 31 percent, and deaths have fallen by 16 percent.
Yet the numbers are still at the horrific highs of November, scientists noted. At least 3,210 people died of Covid-19 on Wednesday alone. And there is no guarantee that these rates will continue to decrease.
“Very, very high case numbers are not a good thing, even if the trend is downward,” said Marc Lipsitch, an epidemiologist at the Harvard T.H. Chan School of Public Health in Boston. “Taking the first hint of a downward trend as a reason to reopen is how you get to even higher numbers.”
In late November, for example, Gov. Gina Raimondo of Rhode Island limited social gatherings and some commercial activities in the state. Eight days later, cases began to decline. The trend reversed eight days after the state’s pause lifted on Dec. 20.
The virus’s latest retreat in Rhode Island and most other states, experts said, results from a combination of factors: growing numbers of people with immunity to the virus, either from having been infected or from vaccination; changes in behavior in response to the surges of a few weeks ago; and a dash of seasonality — the effect of temperature and humidity on the survival of the virus.
Parts of the country that experienced huge surges in infection, like Montana and Iowa, may be closer to herd immunity than other regions. But patchwork immunity alone cannot explain the declines throughout much of the world.
The vaccines were first rolled out to residents of nursing homes and to the elderly, who are at highest risk of severe illness and death. That may explain some of the current decline in hospitalizations and deaths.
But young people drive the spread of the virus, and most of them have not yet been inoculated. And the bulk of the world’s vaccine supply has been bought up by wealthy nations, which have amassed one billion more doses than needed to immunize their populations.
Vaccination cannot explain why cases are dropping even in countries where not a single soul has been immunized, like Honduras, Kazakhstan or Libya. The biggest contributor to the sharp decline in infections is something more mundane, scientists say: behavioral change.
Leaders in the United States and elsewhere stepped up community restrictions after the holiday peaks. But individual choices have also been important, said Lindsay Wiley, an expert in public health law and ethics at American University in Washington.
“People voluntarily change their behavior as they see their local hospital get hit hard, as they hear about outbreaks in their area,” she said. “If that’s the reason that things are improving, then that’s something that can reverse pretty quickly, too.”
The downward curve of infections with the original coronavirus disguises an exponential rise in infections with B.1.1.7, the variant first identified in Britain, according to many researchers.
“We really are seeing two epidemic curves,” said Ashleigh Tuite, an infectious disease modeler at the University of Toronto.
The B.1.1.7 variant is thought to be more contagious and more deadly, and it is expected to become the predominant form of the virus in the United States by late March. The number of cases with the variant in the United States has risen from 76 in 12 states as of Jan. 13 to more than 1,800 in 45 states now. Actual infections may be much higher because of inadequate surveillance efforts in the United States.
Buoyed by the shrinking rates over all, however, governors are lifting restrictions across the United States and are under enormous pressure to reopen completely. Should that occur, B.1.1.7 and the other variants are likely to explode.
Updated
Feb. 25, 2021, 9:03 p.m. ET
“Everybody is tired, and everybody wants things to open up again,” Dr. Tuite said. “Bending to political pressure right now, when things are really headed in the right direction, is going to end up costing us in the long term.”
Another wave may be coming, but it can be minimized.
Looking ahead to late March or April, the majority of scientists interviewed by The Times predicted a fourth wave of infections. But they stressed that it is not an inevitable surge, if government officials and individuals maintain precautions for a few more weeks.
A minority of experts were more sanguine, saying they expected powerful vaccines and an expanding rollout to stop the virus. And a few took the middle road.
“We’re at that crossroads, where it could go well or it could go badly,” said Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases.
The vaccines have proved to be more effective than anyone could have hoped, so far preventing serious illness and death in nearly all recipients. At present, about 1.4 million Americans are vaccinated each day. More than 45 million Americans have received at least one dose.
A team of researchers at Fred Hutchinson Cancer Research Center in Seattle tried to calculate the number of vaccinations required per day to avoid a fourth wave. In a model completed before the variants surfaced, the scientists estimated that vaccinating just one million Americans a day would limit the magnitude of the fourth wave.
“But the new variants completely changed that,” said Dr. Joshua T. Schiffer, an infectious disease specialist who led the study. “It’s just very challenging scientifically — the ground is shifting very, very quickly.”
Natalie Dean, a biostatistician at the University of Florida, described herself as “a little more optimistic” than many other researchers. “We would be silly to undersell the vaccines,” she said, noting that they are effective against the fast-spreading B.1.1.7 variant.
But Dr. Dean worried about the forms of the virus detected in South Africa and Brazil that seem less vulnerable to the vaccines made by Pfizer and Moderna. (On Wednesday, Johnson & Johnson reported that its vaccine was relatively effective against the variant found in South Africa.)
About 50 infections with those two variants have been identified in the United States, but that could change. Because of the variants, scientists do not know how many people who were infected and had recovered are now vulnerable to reinfection.
South Africa and Brazil have reported reinfections with the new variants among people who had recovered from infections with the original version of the virus.
“That makes it a lot harder to say, ‘If we were to get to this level of vaccinations, we’d probably be OK,’” said Sarah Cobey, an evolutionary biologist at the University of Chicago.
Yet the biggest unknown is human behavior, experts said. The sharp drop in cases now may lead to complacency about masks and distancing, and to a wholesale lifting of restrictions on indoor dining, sporting events and more. Or … not.
“The single biggest lesson I’ve learned during the pandemic is that epidemiological modeling struggles with prediction, because so much of it depends on human behavioral factors,” said Carl Bergstrom, a biologist at the University of Washington in Seattle.
Taking into account the counterbalancing rises in both vaccinations and variants, along with the high likelihood that people will stop taking precautions, a fourth wave is highly likely this spring, the majority of experts told The Times.
Kristian Andersen, a virologist at the Scripps Research Institute in San Diego, said he was confident that the number of cases will continue to decline, then plateau in about a month. After mid-March, the curve in new cases will swing upward again.
In early to mid-April, “we’re going to start seeing hospitalizations go up,” he said. “It’s just a question of how much.”
Summer will feel like summer again, sort of.
Now the good news.
Despite the uncertainties, the experts predict that the last surge will subside in the United States sometime in the early summer. If the Biden administration can keep its promise to immunize every American adult by the end of the summer, the variants should be no match for the vaccines.
Combine vaccination with natural immunity and the human tendency to head outdoors as weather warms, and “it may not be exactly herd immunity, but maybe it’s sufficient to prevent any large outbreaks,” said Youyang Gu, an independent data scientist, who created some of the most prescient models of the pandemic.
Infections will continue to drop. More important, hospitalizations and deaths will fall to negligible levels — enough, hopefully, to reopen the country.
“Sometimes people lose vision of the fact that vaccines prevent hospitalization and death, which is really actually what most people care about,” said Stefan Baral, an epidemiologist at the Johns Hopkins Bloomberg School of Public Health.
Even as the virus begins its swoon, people may still need to wear masks in public places and maintain social distance, because a significant percent of the population — including children — will not be immunized.
“Assuming that we keep a close eye on things in the summer and don’t go crazy, I think that we could look forward to a summer that is looking more normal, but hopefully in a way that is more carefully monitored than last summer,” said Emma Hodcroft, a molecular epidemiologist at the University of Bern in Switzerland.
Imagine: Groups of vaccinated people will be able to get together for barbecues and play dates, without fear of infecting one another. Beaches, parks and playgrounds will be full of mask-free people. Indoor dining will return, along with movie theaters, bowling alleys and shopping malls — although they may still require masks.
The virus will still be circulating, but the extent will depend in part on how well vaccines prevent not just illness and death, but also transmission. The data on whether vaccines stop the spread of the disease are encouraging, but immunization is unlikely to block transmission entirely.
“It’s not zero and it’s not 100 — exactly where that number is will be important,” said Shweta Bansal, an infectious disease modeler at Georgetown University. “It needs to be pretty darn high for us to be able to get away with vaccinating anything below 100 percent of the population, so that’s definitely something we’re watching.”
Over the long term — say, a year from now, when all the adults and children in the United States who want a vaccine have received them — will this virus finally be behind us?
Every expert interviewed by The Times said no. Even after the vast majority of the American population has been immunized, the virus will continue to pop up in clusters, taking advantage of pockets of vulnerability. Years from now, the coronavirus may be an annoyance, circulating at low levels, causing modest colds.
Many scientists said their greatest worry post-pandemic was that new variants may turn out to be significantly less susceptible to the vaccines. Billions of people worldwide will remain unprotected, and each infection gives the virus new opportunities to mutate.
“We won’t have useless vaccines. We might have slightly less good vaccines than we have at the moment,” said Andrew Read, an evolutionary microbiologist at Penn State University. “That’s not the end of the world, because we have really good vaccines right now.”
For now, every one of us can help by continuing to be careful for just a few more months, until the curve permanently flattens.
“Just hang in there a little bit longer,” Dr. Tuite said. “There’s a lot of optimism and hope, but I think we need to be prepared for the fact that the next several months are likely to continue to be difficult.”